Giorgio Bedogni 1, Paolo Brambilla 2, Stefano Bellentani 1 and Claudio Tiribelli 1
1 Liver Research Center, Basovizza, Trieste, and Italian Liver Trust, Campogalliano, Modena, Italy.
2 International Center for the Assessment of Nutritional Status (ICANS), University of Milano, Milano, Italy.
Running title: body composition in heath and disease
Keywords: body composition, reference methods, indirect methods, health, disease
1. Abstract
Body composition (BC) is the best long-term indicator of nutritional status and it is of interest to physicians and researchers because of its association with health status. The assessment of BC involves the use of multicompartment models that are not readily available in clinical practice and epidemiological research. Indirect methods, i.e. methods making use of predictive algorithms, are often used in these settings. However, while the use of BC algorithms may be accurate at the population level, it rarely is at the individual level. Albeit not yet a gold-standard technique, dual-energy x-ray absorptiometry holds significant promise for the assessment BC in clinical practice and epidemiological studies. Anthropometry is the single most universally applicable and inexpensive BC method and is of great importance because of its association with health status. Bioelectrical impedance analysis is an indirect BC technique that may be of interest for the study of body water distribution between extra- and intra-cellular spaces.
2. Body composition and nutritional status
Nutritional status can be operationally thought as resulting from the interaction of body composition (BC), energy balance and body functionality (Figure 1) (Bedogni et al. 1999). BC is the best long-term indicator of nutritional status and it is of interest to clinicians and researchers mainly because of its association with body functionality. It is this latter, in fact, as shown by Figure 1, to provide the most important link between nutritional status and health status.
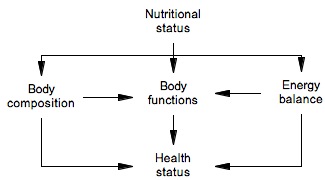
Figure 1
Operational definition of nutritional status (Bedogni et al. 1999).
3. The molecular model of body composition
Body composition can be studied at five levels: atomic, molecular, cellular, organ and tissue, and whole-body (Heymsfield et al. 1997). The molecular level of body composition is depicted in Figure 2 (Bedogni et al. 1999).

Figure 2
Body composition of the reference man (Bedogni et al. 1999). Abbreviations: BW = body weight; FFM = fat-free mass; FM = fat-mass; TBW = total body water; PM = protein mass; MM = mineral mass; Gn = glycogen; FM = fat mass. See text for details.
At this level, body weight (BW) is the sum of total body water (TBW), protein mass (PM), mineral mass (MM), glycogen (Gn) and fat mass (FM) (Heymsfield et al. 1997). TBW is most commonly measured by 2H2O or 3H2O dilution, PM is obtained from total body nitrogen measured by neutron activation analysis, and the osseous part of mineral mass by dual-energy x-ray absorptiometry (DXA). Although Gn is not of great interest to the student of body composition because of its intrinsic lability, it can nonetheless be measured by 13C magnetic resonance spectroscopy. TBW can be further separated into extracellular (ECW) and intracellular water (ICW). ICW is of special interest to the body compositionist because of the possibility of using it as an indicator of cellular health status (Bedogni et al. 2003). ICW cannot be measured directly but only by subtracting ECW - most commonly assessed by bromide dilution - from TBW (Heymsfield et al. 1997).
4. Two-compartment models of body composition
The sum of TBW, PM, MM and Gn makes up the so-called fat-free mass (FFM). Two-compartment (2C) BC models consider BW as the sum of FFM and FM, deliberately ignoring the heterogeneity of the former (Figure 2) (Bedogni et al. 1999). When this approximation is acceptable, BC can be assessed by measuring a physical or chemical property of FFM which is in constant relationship with FFM itself. The 2C models are body densitometry, 40K measurement, and TBW measurement (Heymsfield et al. 1997). Body densitometry measures body density by underwater weighing or air plethysmograhy and then estimates BC assuming of a constant density of FFM and FM (1.1000 kg*L-1 and 0.9007 kg*L-1 respectively for the “reference man”). Measurement of the natural isotope of potassium 40K by means of γ-counters allows to estimate total body potassium (TBK) because of their constant ratio inside the human body; FFM is then estimated from the potassium content of FFM (68 mEq*kg-1 in the reference man). Lastly, measurement of TBW by 2H2O or 3H2O dilution allows to estimate FFM if the hydration of the latter is known (73% in the reference man).
5. Three- and four-compartment models of body composition
Of the four components of FFM, TBW and the osseous component of MM are much easier to measure than PM and Gn. Because FFM density is the sum of the densities of its four components, it is intuitive that the correction of body density for TBW and / or MM offers a more accurate assessment of FFM than body density alone. Indeed, four-compartment (4C) models based on the measurement of body density, TBW and MM are considered gold-standard BC models, even if they are obviously less accurate than the molecular model (Heymsfield et al. 1997).
6. Effects of gender, growth and aging on body composition
Qualitative changes of BC occurring during life are similar in males and females. However, BC differs quantitatively in males and females at all ages of life (Fomon et al. 1982; Hascke 1983; Forbes 1987). During growth, females show a greater development of FM and a slower maturation of FFM than males (Figures 3 and 4) (Bedogni et al. 1999).

Figure 3
Changes of FFM composition from birth to 10 years of age (Bedogni et al. 1999). Abbreviations: TBW = total body water; ICW = intracellular water; ECW = extracellular water; PM = protein mass; MM = mineral mass. Black and white points represent males and females, respectively. Graphs were plotted from the data of Fomon et al. (1982).
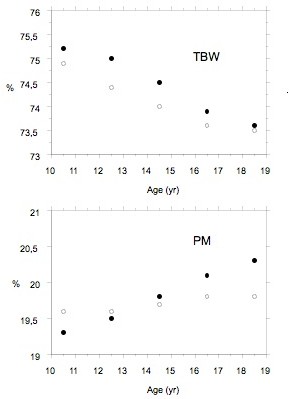
Figure 4
Changes in water and protein content of fat-free mass from 10 to 18 years of age (Bedogni et al. 1999). Abbreviations: TBW = total body water; PM = Protein mass. Black and white points represent males and females, respectively. Graphs were plotted from the data of Hascke (1983).
FFM hydration decreases from about 80% at birth to 73% in adulthood. The few available studies suggest the latter value persists also during elderly. It is of some interest that at about two years of age, ICW starts to prevail on ECW inside FFM, offering an indirect indication of cellular growth. PM increases substantially from birth to two years of age and at about 18 years reaches its mature value of 20%. As an absolute value, PM is lower in elderly than in adult subjects. An interesting fact about MM during growth is its slower increase in females as compared to males. A decrease in MM occurs virtually always during aging. The dimensions of the body compartments in Figure 1 are those of the “reference man”. The definition of a “reference woman” is more complicated because much less data are available. It is generally agreed, however, that the reference woman has 12% more FM than the reference man (and thus 12% less FFM) (Forbes 1987).
7. Effects of disease on body composition
Even if many diseases have peculiar effects on BC, some general effects of disease on BC can be delineated (Jeejeebhoy 1996). First of all, an illness able to negativize energy balance for a long period produces not only a contraction of FM but also of FFM. ECW modifications are often evident, e.g. edema signals ECW expansion and a high hematocrit may be a sign of ECW contraction. ICW modifications are much less evident than those of ECW but are of great interest because they provide a way to assess cellular health status (Bedogni et al. 2003). An expansion of ICW is common to many diseases and often depends from malfunctioning of membrane ionic pumps. A contraction of ICW:TBW signals a cellular suffering mostly determined by osmotic factors. Leanness and obesity are defined respectively as a deficit and as an excess of FM. Both, however, are associated to important changes inside FFM. The majority of obese individuals have in fact also an expanded TBW, ECW, PM and MM. Interestingly, the expansion of ECW:TBW is seen in both young and adult subjects and persists after weight loss (Mazariegos et al. 1992; Battistini et al. 1995; Marken Lichtenbelt and Fogelholm 1999). Sarcopenic obesity, i.e. obesity accompanied by low FFM, is rare and often of genetic origin (Brambilla et al. 1997).
8. Indirect assessment of body composition
The use of multicompartment models of BC has increased our knowledge of the mechanisms of growth, aging and disease. However, the complexity, invasiveness and cost of multicompartment models hinder their use in clinical practice and epidemiological studies (Heymsfield et al. 1997). Indirect BC techniques employ predictive equations to estimate a body compartment from an easily quantifiable characteristic (e.g. FM from skinfolds). A predictive equation must always be evaluated using both statistical and practical criteria (Guo et al. 1996). These criteria include: 1) consideration of the known population-specificity of predictive algorithms, 2) critical evaluation of the contribution of each predictor incorporated in the equation and, most important from a practical viewpoint, 3) total and individual error. BC equations - as all algorithms - are often accurate at the population level but not at the individual level. This limits the use of indirect methods in clinical practice but they have great potential for epidemiological use.
9. Anthropometry
As stated by the World Health Organization, “Anthropometry is the single most universally applicable, inexpensive and non-invasive method to assess the size, proportions, and composition of the human body” (World Health Organization 1995). The importance of anthropometry stems from its strict association with body functionality. For instance, body mass index (BMI) is employed in clinical and research practice not because it is a good predictor of FM (Bedogni et al. 2001) but because it is a reasonably accurate predictor of the risk of disease (World Health Organization 1998). Similarly, waist circumference is not an accurate predictor of visceral adipose tissue but is a reasonably accurate predictor of the risk of disease, independently from BMI (World Health Organization 1998). The interpretation of BMI and WC should always consider the ethnic group and the fact that the commonly quoted reference values apply to Caucasian people only (World Health Organization 1998; World Health Organization Expert Committee 2004).
10. Bioelectrical impedance analysis
Bioelectrical impedance analysis (BIA) is an indirect technique for the assessment of TBW and of its distribution between ECW and ICW (Deurenberg 1994; National Institutes of Health 1996). The underlying principle of BIA is that an alternating electrical current (a.c.) cannot pass cell membranes at low frequencies (≤ 5 kHz) while it is able to penetrate cells at higher frequencies (≥ 100 kHz). Thus, BIA provides an estimate of ECW and TBW, i.e. ECW + ICW, at low and high frequencies, respectively. BIA provides also a way of estimating FFM because TBW makes the most part of FFM (see Figure 1). Moreover, segmental BIA has a great potential for the assessment of appendicular BC, especially in relation to the prognostic significance of sarcopenia (Malavolti et al. 2003).
11. DXA
DXA is the recognized gold-standard for the assessment of bone mineral content (BMC). The 3-compartment DXA model separates body mass into FM, lean tissue mass (LTM) and bone mineral content (BMC), with the sum of LTM and BMC representing fat-free mass (FFM) (Pietrobelli et al. 1996). Moreover, at the appendicular level, LTM is synonym with skeletal muscle mass so that DXA provides a simple means of evaluating skeletal muscle mass (Malavolti et al. 2003). Even if DXA should not be considered as a gold-standard, also owing to the fact that different densitometers and software versions give different estimates of BC, it has a great potential because it is more available than other BC methods and is being increasingly studied against clinical and health outcomes.
12. Conclusion
The assessment of BC is central to the evaluation of patients with nutritional problems and to the assessment of the status of health of populations. Multicompartment models of BC are useful to study the mechanisms of growth, aging and disease, but they are replaced by indirect methods or functionally relevant indicators in clinical and epidemiological settings.
13. References
Battistini, N., Virgili, F., Severi, S., Brambilla, P., Manzoni, P., et al.: Relative expansion of extracellular water in obese vs. normal children. J Appl Physiol 79: 94-96 (1995).
Bedogni, G., Battistini, N. and Borghi, A.: [Principles of Nutritional Assessment]. EDRA, Milano, Italy (1999).
Bedogni, G., Borghi, A. and Battistini, N.: Body water distribution and disease. Acta Diabetol 40 Suppl 1: S200-202 (2003).
Bedogni, G., Pietrobelli, A., Heymsfield, S. B., Borghi, A., Manzieri, A. M., et al.: Is body mass index a measure of adiposity in elderly women? Obes Res 9: 17-20 (2001).
Brambilla, P., Bosio, L., Manzoni, P., Pietrobelli, A., Beccaria, L., et al.: Peculiar body composition in patients with Prader-Labhart-Willi syndrome. Am J Clin Nutr 65: 1369-1374 (1997).
Deurenberg, P.: International consensus conference on impedance in body composition. Age Nutr 5: 142-145 (1994).
Fomon, S., Haschke, F., Ziegler, E. and Nelson, S.: Body composition of reference children from birth to age 10 years. Am J Clin Nutr: 35: 1169-1175 (1982).
Forbes, G. B.: Human Body Composition. Growth, Aging, Nutrition and Activity Springer-Verlag, NY (1987).
Guo, S., Chumlea, W. and Cockram, D.: Use of statistical methods to estimate body composition. Am J Clin Nutr: 428S-435S (1996).
Hascke, F.: Body composition of adolescent males. Part I: total body water in normal adolescent males. Acta Ped Scand Suppl. 307: 1-23 (1983).
Heymsfield, S. B., Wang, Z., Baumgartner, R. N. and Ross, R.: Human body composition: advances in models and methods. Annu Rev Nutr 17: 527-58 (1997).
Jeejeebhoy, K. N: Body composition in weight loss and pathological states. In: Human Body Composition, pp. 275-283, Roche A. F., Heymsfield S. B. and Lohman T. G. (Eds.) Human Champaign, Human Kinetics (1996).
Malavolti, M., Mussi, C., Poli, M., Fantuzzi, A. L., Salvioli, G., et al.: Cross-calibration of eight-polar bioelectrical impedance analysis versus dual-energy X-ray absorptiometry for the assessment of total and appendicular body composition in healthy subjects aged 21-82 years. Ann Hum Biol 30: 380-391 (2003).
Marken Lichtenbelt, W. D. and Fogelholm, M.: Increased extracellular water compartment, relative to intracellular water compartment, after weight reduction. J Appl Physiol 87: 294-298 (1999).
Mazariegos, M., Kral, J. G., Wang, J., Waki, M., Heymsfield, S. B., et al.: Body composition and surgical treatment of obesity. Effects of weight loss on fluid distribution. Ann Surg 216: 69-73 (1992).
National Institutes of Health (NIH): Bioelectrical impedance analysis in body composition measurement. Am J Clin Nutr 64 (Suppl): 387S-531S (1996).
Pietrobelli, A., Formica, C., Wang, Z. and Heymsfield, S.: Dual-energy X-ray absorptiometry body composition model: review of physical concepts. Am J Physiol: E941-E951 (1996).
World Health Organization: Physical status: the use and interpretation of anthropometry. World Health Organization, Geneva (1995).
World Health Organization: Obesity: preventing and managing the global epidemic. World Health Organization, Geneva (1998).
World Health Organization Expert Committee: Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet 363: 157-163 (2004).